
- Home
- About
- Portfolio
Crush the Match – Medical School and Residency Platform
Food¢ense – Curbing Childhood Obesity and Food Waste
HealthStack – Shared and Jailed HIPAA Hosting $50
Marta Care – Let Us Help When You Can’t
MD Idea Lab – We Build Prototypes for Doctors
Nervcell – The Healthcare Web Browser
Patient Keto – Personalized Keto Medicine and Telehealth
SwipeChart – Rapid EMR Interface
Treatment Scores – Quantifying the Science of Medicine
Treatments – Diagnosed. Now What?
VIDRIO – Google Glass and EMR Interface
- Blog
- Contact
Blog
Follow our blog and stay up to date.
The Role of Health Informatics in Healthcare: Why Healthcare Providers Should Become Proficient
by Stephen Fitzmeyer, MD
Health informatics is a rapidly growing field that combines healthcare, information technology, and data analysis to improve the quality and efficiency of healthcare delivery. It involves the use of technology and information systems to collect, store, and analyze patient data, enabling healthcare providers to make informed decisions about patient care. In this article, we will discuss what health informatics is, how it is useful, and why healthcare providers should become proficient in it.
What is Health Informatics?
Health informatics is the field of study that focuses on the use of technology and information systems to manage healthcare data. It involves the collection, storage, analysis, and dissemination of healthcare data to support decision-making in healthcare delivery. Health informatics professionals are responsible for developing and implementing information systems that support healthcare providers in delivering high-quality care to patients.
How is Health Informatics Useful?
Health informatics is useful in healthcare in several ways. First, it enables healthcare providers to collect and store patient data electronically, reducing the risk of errors and improving the accuracy of patient records. This also allows for easier and faster access to patient data, enabling healthcare providers to make informed decisions about patient care.
Second, health informatics facilitates communication and collaboration among healthcare providers. Electronic health records (EHRs) and other health information systems allow healthcare providers to share patient data with each other, enabling them to work together more effectively to develop and implement treatment plans.
Third, health informatics supports evidence-based practice. By analyzing patient data, healthcare providers can identify patterns and trends that can inform clinical decision-making and improve patient outcomes. Health informatics also enables healthcare providers to access the latest research and best practices, supporting evidence-based practice.
Why Should Healthcare Providers Become Proficient in Health Informatics?
Healthcare providers should become proficient in health informatics for several reasons. First, proficiency in health informatics enables healthcare providers to make informed decisions about patient care. By understanding how to access and analyze patient data, healthcare providers can develop treatment plans that are tailored to individual patient needs and are based on the latest research and best practices.
Second, proficiency in health informatics supports collaboration and communication among healthcare providers. By understanding how to use health information systems, healthcare providers can share patient data with each other more effectively, enabling them to work together to develop and implement treatment plans.
Third, proficiency in health informatics supports the transition to value-based care. As healthcare moves towards a value-based care model, healthcare providers need to understand how to use health information systems to collect and analyze data on patient outcomes. By understanding how to use health informatics to support evidence-based practice and measure patient outcomes, healthcare providers can demonstrate the value of their services and improve patient outcomes.
In conclusion, health informatics is a rapidly growing field that plays a critical role in healthcare delivery. Healthcare providers who become proficient in health informatics can improve the quality and efficiency of healthcare delivery, supporting evidence-based practice and the transition to value-based care. By investing in health informatics education and training, healthcare providers can position themselves to provide high-quality care and improve patient outcomes.
Author: Stephen Fitzmeyer, M.D.
Physician Informaticist
Founder of Patient Keto
Founder of Warp Core Health
Founder of Jax Code Academy, jaxcode.com
Connect with Dr. Stephen Fitzmeyer:
Twitter: @PatientKeto
LinkedIn: linkedin.com/in/sfitzmeyer/

Unveiling the Mathematics of Epidemiology: Analyzing Disease Patterns and Prevention Strategies
Epidemiology, the scientific study of health and disease distribution in populations, is a field that relies on mathematical concepts and analysis to understand and combat public health challenges. In this article, we will explore some key mathematical examples that highlight the significance of epidemiology in healthcare.
Incidence and Prevalence: Let’s consider a hypothetical population of 10,000 individuals. Over the course of one year, 500 new cases of a particular disease are diagnosed. The incidence of the disease in this population would be calculated as follows:
Incidence = (Number of new cases / Total population) x 1,000 Incidence = (500 / 10,000) x 1,000 Incidence = 50 cases per 1,000 population
Prevalence, on the other hand, measures the proportion of individuals with the disease at a specific point in time. If, at the beginning of the year, there were already 200 existing cases in the population, the prevalence of the disease would be:
Prevalence = (Number of existing cases / Total population) x 1,000 Prevalence = (200 / 10,000) x 1,000 Prevalence = 20 cases per 1,000 population
These calculations provide healthcare providers with valuable information about the disease burden and help in identifying trends and potential risk factors.
Risk Factors: Let’s consider a study examining the relationship between smoking and the development of lung cancer. Researchers gather data from a sample of 1,000 individuals, finding that 300 of them are smokers and 100 of those smokers develop lung cancer over a five-year period. The incidence rate of lung cancer among smokers can be calculated as:
Incidence Rate = (Number of new cases among smokers / Total number of smokers) x 1,000 Incidence Rate = (100 / 300) x 1,000 Incidence Rate = 333.33 cases per 1,000 smokers
This example demonstrates how epidemiology can quantify the association between a specific risk factor (smoking) and the occurrence of a disease (lung cancer).
Outbreak Investigation: During an outbreak investigation, data collection and analysis are crucial for identifying the source and mode of transmission of a disease. Let’s say there is an outbreak of a foodborne illness, and investigators collect information from 500 affected individuals. By analyzing the data, they find that 400 of them consumed a particular brand of contaminated food. This finding suggests a potential association between the contaminated food and the outbreak.
Screening: To illustrate the importance of screening, let’s consider a population of 2,000 individuals eligible for a breast cancer screening program. The screening test has a sensitivity of 90% and a specificity of 95%. Out of the 50 individuals who have breast cancer, 45 will test positive (true positives) while 5 will test negative (false negatives). Out of the 1,950 individuals without breast cancer, 1,852 will test negative (true negatives) while 98 will test positive (false positives). These numbers highlight the trade-off between identifying true cases of breast cancer and the potential for false-positive results.
Clinical Trials: Clinical trials rely on statistical analysis to assess the effectiveness of new treatments or interventions. For instance, a study involving 500 participants might randomly assign half of them to receive a new medication while the other half receives a placebo. By comparing the outcomes between the two groups, researchers can determine the efficacy of the medication and make evidence-based decisions regarding its use in clinical practice.
By understanding these mathematical examples within the context of epidemiology, healthcare providers can gain valuable insights into the distribution and determinants of diseases. This knowledge enables them to develop effective prevention and control strategies, improve population health outcomes,
and make informed decisions in healthcare. The application of mathematics in epidemiology provides a quantitative framework for understanding the patterns and dynamics of diseases within populations.
Mathematics allows us to quantify the incidence and prevalence of diseases, providing a measure of the disease burden and helping healthcare providers allocate resources effectively. By calculating incidence rates, we can assess the risk factors associated with diseases, such as the relationship between smoking and lung cancer.
During outbreaks, mathematical analysis helps investigators identify the source and mode of transmission of diseases, guiding public health interventions to prevent further spread. Screening programs utilize mathematical concepts to evaluate the performance of tests, balancing the need for early detection with the risk of false positives.
Clinical trials, powered by statistical analysis, provide evidence-based information on the efficacy and safety of new treatments. Mathematics helps determine sample sizes, assess treatment outcomes, and draw valid conclusions about the effectiveness of interventions.
The integration of mathematics in epidemiology strengthens the foundation of public health decision-making. It allows healthcare providers to make data-driven assessments, identify high-risk populations, implement targeted interventions, and monitor the impact of preventive measures.
As we continue to navigate the challenges of disease prevention and control, understanding the role of mathematics in epidemiology is paramount. By harnessing the power of numbers, healthcare providers can effectively analyze and interpret health data, paving the way for evidence-based strategies that protect and promote the well-being of populations.
Author: Stephen Fitzmeyer, M.D.
Physician Informaticist
Founder of Patient Keto
Founder of Warp Core Health
Founder of Jax Code Academy, jaxcode.com
Connect with Dr. Stephen Fitzmeyer:
Twitter: @PatientKeto
LinkedIn: linkedin.com/in/sfitzmeyer/
Probiotics as Adjunctive Treatment for Depression: A Promising Frontier
Introduction
Depression is a prevalent and debilitating mental health disorder that affects millions of people worldwide. While current treatment options such as antidepressant medication and psychotherapy can be effective, a significant proportion of individuals with depression do not experience a satisfactory response. This has led researchers to explore novel approaches to treatment, and one such area of investigation is the use of probiotics. Probiotics, which are live microorganisms that confer health benefits when consumed, have shown promise in influencing the microbiota-gut-brain axis and improving depressive symptoms. A recent pilot randomized clinical trial published in JAMA Psychiatry by Nikolova et al. (2023) investigated the acceptability, tolerability, and potential efficacy of probiotics as an adjunctive treatment for depression. The study’s findings shed light on the potential benefits of probiotics and provide a basis for further investigation in larger efficacy trials.
Study Overview
The study conducted by Nikolova et al. included 49 participants with major depressive disorder (MDD) who had an incomplete response to antidepressant medication. The participants were randomly assigned to receive either a multistrain probiotic or a placebo in addition to their ongoing antidepressant treatment. The trial lasted for 8 weeks, during which the researchers assessed various outcomes, including depressive and anxiety symptoms, treatment adherence, tolerability, and adverse reactions.
Key Findings
The results of the study revealed several important findings. Firstly, the probiotic group demonstrated greater improvements in depressive and anxiety symptoms compared to the placebo group. This was evident from the reduction in scores on rating scales such as the Hamilton Depression Rating Scale (HAMD-17), Inventory of Depressive Symptomatology (IDS), Hamilton Anxiety Rating Scale (HAMA), and General Anxiety Disorder (GAD-7). Secondly, the probiotic intervention was well-tolerated, with a high adherence rate and no serious adverse reactions reported. The dropout rate was low, further highlighting the acceptability of probiotics as a treatment option. Finally, the effect sizes observed in the probiotic group were moderate, suggesting a potential therapeutic benefit.
Implications and Future Directions
The findings of this pilot trial provide a solid foundation for further investigation of probiotics as adjunctive treatment for individuals with major depressive disorder. The acceptability, tolerability, and estimated effect sizes on key clinical outcomes indicate that probiotics may offer a promising avenue for improving depressive symptoms. However, it is important to note that this study was a pilot trial with a relatively small sample size, and thus, larger efficacy trials are needed to confirm and build upon these preliminary findings.
The potential mechanisms through which probiotics exert their effects on depressive symptoms are still being explored. The microbiota-gut-brain axis is thought to play a crucial role in influencing mood and behavior, and probiotics may modulate this axis by promoting a healthy gut microbiome. Further research is required to elucidate the specific strains and dosages of probiotics that are most effective in treating depression, as well as to identify the patient subgroups that may benefit the most from this intervention.
Conclusion
Depression is a complex and multifaceted condition that demands innovative treatment approaches. The study by Nikolova et al. contributes to the growing body of evidence supporting the potential use of probiotics as adjunctive treatment for depression. The results demonstrate the acceptability, tolerability, and estimated effect sizes of probiotics in improving depressive and anxiety symptoms. These findings underscore the need for larger, well-designed efficacy trials to confirm the therapeutic potential of probiotics and inform clinical practice. If future studies continue to show promising results, probiotics could represent a safe, accessible, and scalable treatment option for individuals with depression, complementing existing interventions and improving patient outcomes.
Reference Article:
Title: Acceptability, Tolerability, and Estimates of Putative Treatment Effects of Probiotics as Adjunctive Treatment in Patients With Depression: A Randomized Clinical Trial Journal: JAMA Psychiatry Date: June 14, 2023
Author: Stephen Fitzmeyer, M.D.
Physician Informaticist
Founder of Patient Keto
Founder of Warp Core Health
Founder of Jax Code Academy, jaxcode.com
Connect with Dr. Stephen Fitzmeyer:
Twitter: @PatientKeto
LinkedIn: linkedin.com/in/sfitzmeyer/

Understanding the Fundamental Concepts of Epidemiology in Healthcare
By Stephen Fitzmeyer, MD
Epidemiology is the study of the distribution and determinants of health and disease in populations. It is a critical field in healthcare that helps healthcare providers understand the patterns and causes of diseases and develop strategies to prevent and control them. In this article, we will discuss some of the fundamental concepts of epidemiology in healthcare.
Incidence and Prevalence: Incidence is the number of new cases of a disease in a population over a specified period of time. Prevalence is the proportion of individuals in a population with a particular disease at a given point in time. These measures help healthcare providers understand the burden of a disease in a population and the risk factors associated with it.
Risk Factors: Risk factors are the characteristics or behaviors that increase the likelihood of developing a disease. They can be divided into two categories: modifiable and non-modifiable. Modifiable risk factors, such as smoking and poor diet, can be changed to reduce the risk of developing a disease. Non-modifiable risk factors, such as age and genetics, cannot be changed.
Outbreak Investigation: When a disease outbreak occurs, it is important to investigate the outbreak to determine the source of the disease and prevent further spread. Outbreak investigations involve identifying the affected population, collecting data on the disease, and analyzing the data to identify the source and mode of transmission of the disease.
Screening: Screening is the process of testing individuals who do not have any symptoms of a disease to identify those who may be at risk. Screening tests are used to detect diseases at an early stage when treatment is most effective. However, screening tests can also have risks, such as false-positive results, which can lead to unnecessary interventions and anxiety.
Clinical Trials: Clinical trials are research studies that evaluate the safety and effectiveness of new treatments or interventions. They are critical in healthcare as they provide evidence-based information on the efficacy and safety of treatments, which can inform clinical practice.
Understanding these fundamental concepts of epidemiology is crucial in healthcare, as they inform the development of prevention and control strategies for diseases. Epidemiology helps healthcare providers identify the risk factors associated with a disease, develop screening and prevention programs, and evaluate the effectiveness of interventions. By applying these concepts, healthcare providers can work towards improving the health of populations and reducing the burden of disease.
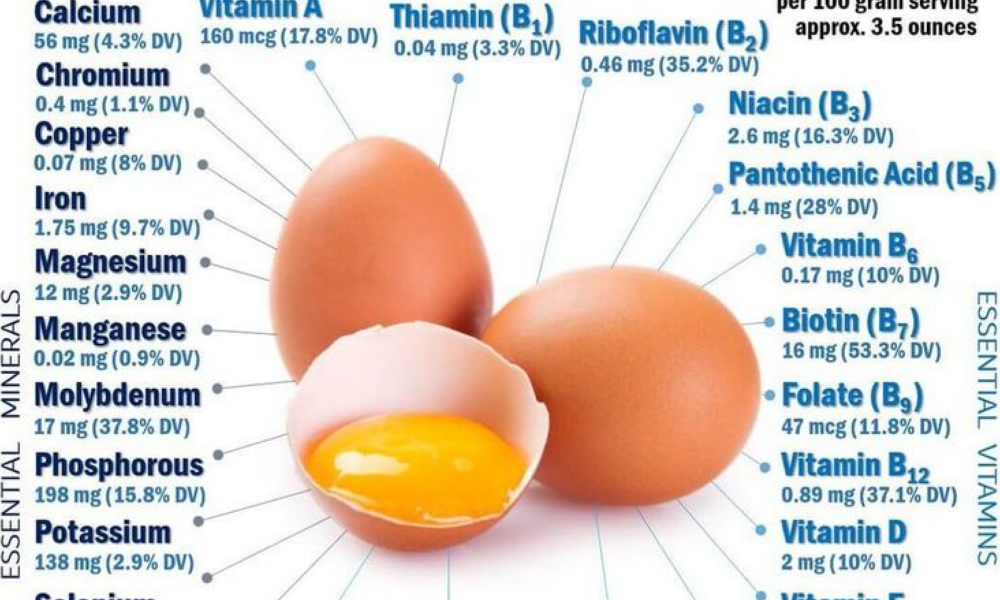
Eggs: The Superfood for a Ketogenic Diet
When it comes to the ketogenic diet, few foods are as versatile and beneficial as eggs. These little powerhouses are packed with essential nutrients and can play a significant role in your journey towards achieving ketosis and optimizing your health. From providing high-quality protein to a wealth of vitamins and minerals, eggs offer numerous benefits that make them an ideal choice for those following a ketogenic lifestyle.
Protein Powerhouse: One of the key components of a ketogenic diet is consuming an adequate amount of protein to support muscle growth, repair, and overall health. Eggs are a complete protein source, containing all nine essential amino acids that our bodies need but cannot produce on their own. Adding eggs to your ketogenic meal plan ensures you’re getting a high-quality protein source to nourish your body.
Healthy Fats: While the ketogenic diet is known for its emphasis on fats, it’s crucial to choose healthy sources. Eggs provide a perfect balance of fats, including heart-healthy monounsaturated and polyunsaturated fats. They are also an excellent source of omega-3 fatty acids, which have anti-inflammatory properties and are essential for brain health.
Micronutrient Marvels: Eggs are a nutrient-dense food, offering a wide range of essential vitamins and minerals that support overall well-being. They are rich in:
- Vitamin A: Essential for eye health and immune function.
- Vitamin D: Important for bone health and immune system support.
- Vitamin E: An antioxidant that protects cells from damage.
- Vitamin B12: Vital for brain function and energy production.
- Vitamin B6: Helps convert food into energy and supports brain health.
- Riboflavin (Vitamin B2): Plays a key role in energy metabolism.
- Folate (Vitamin B9): Important for DNA synthesis and cell growth.
- Iron: Essential for oxygen transport and energy production.
- Selenium: Acts as an antioxidant and supports thyroid function.
Appetite Control: One of the advantages of eggs on a ketogenic diet is their ability to keep you feeling full and satisfied. Due to their high protein and healthy fat content, eggs help curb hunger and prevent overeating. Incorporating eggs into your meals can assist in appetite control, making it easier to adhere to your ketogenic eating plan.
Versatility in Cooking: Eggs are incredibly versatile and can be enjoyed in numerous ways. From scrambled and poached to boiled and omelets, there’s a variety of delicious ways to incorporate eggs into your ketogenic meals. You can also use eggs as a binding agent in recipes or create low-carb keto-friendly baked goods.
In addition to their nutritional benefits, eggs offer the advantage of being a food you can enjoy without concern about quantity. Unlike many other foods, you can eat eggs in larger quantities without worrying about derailing your ketogenic goals. Their high protein and healthy fat content make them a satisfying choice that can help you stay on track with your dietary plan.
So go ahead and embrace the wonders of eggs on your ketogenic journey! Enjoy them as part of your meals, snacks, and recipes, knowing that they provide an array of essential nutrients to support your health and well-being. Whether you prefer them scrambled, boiled, or in an omelet, eggs are a guilt-free choice that can be savored without limits.
Remember, if you have any specific health concerns or dietary restrictions, it’s always a good idea to consult with a healthcare professional or registered dietitian for personalized guidance.
Author: Stephen Fitzmeyer, M.D.
Physician Informaticist
Founder of Patient Keto
Founder of Warp Core Health
Founder of Jax Code Academy, jaxcode.com
Connect with Dr. Stephen Fitzmeyer:
Twitter: @PatientKeto
LinkedIn: linkedin.com/in/sfitzmeyer/

The Vegan/Vegetarian Guide to Following a Ketogenic Diet with Intermittent Fasting
Introduction: The ketogenic diet has gained popularity for its potential benefits in weight loss, improved metabolic health, and increased energy levels. However, individuals following a vegan or vegetarian lifestyle might wonder if it’s possible to adopt a ketogenic diet without compromising their dietary preferences. The good news is that with careful planning and consideration, vegans and vegetarians can successfully incorporate the principles of a ketogenic diet while practicing intermittent fasting.
Understanding the Ketogenic Diet: A ketogenic diet is characterized by a significant reduction in carbohydrate intake and an increased consumption of healthy fats. The aim is to shift the body’s primary fuel source from carbohydrates to fat, resulting in a metabolic state known as ketosis. This switch allows the body to burn stored fat for energy instead of relying on glucose from carbohydrates.
Key Principles for Vegans and Vegetarians: While traditional ketogenic diets often rely heavily on animal-based products, vegan and vegetarian versions can be equally effective and satisfying. Here are some key principles to follow:
- Plant-Based Fats: Incorporate healthy fats from plant sources such as avocados, coconut oil, olive oil, nuts, and seeds. These provide essential nutrients, promote satiety, and support the ketogenic state.
- Non-Starchy Vegetables: Fill your plate with a variety of low-carbohydrate, non-starchy vegetables like leafy greens, cruciferous vegetables, zucchini, cauliflower, and bell peppers. These provide essential vitamins, minerals, and fiber while keeping carbohydrate intake low.
- Protein Alternatives: For vegetarians, include high-quality protein sources like eggs, dairy products, and plant-based protein options such as tofu, tempeh, seitan, and legumes. Vegans can rely on plant-based proteins like tofu, tempeh, legumes, quinoa, and hemp seeds.
- Healthy Snacks: Choose keto-friendly snacks like nuts, seeds, olives, coconut chips, or homemade energy balls using low-carb ingredients. These snacks help maintain energy levels and keep you satisfied between meals.
Incorporating Intermittent Fasting: Intermittent fasting (IF) can complement a ketogenic diet by optimizing insulin sensitivity and enhancing fat-burning processes. Here are two popular approaches:
- Time-Restricted Eating: Choose a daily eating window, such as 16/8, where you fast for 16 hours and eat all your meals within an 8-hour window. Adjust the timing to suit your lifestyle and preferences.
- Alternate-Day Fasting: This method involves fasting on alternate days, with reduced calorie intake or fasting for a full 24 hours. On non-fasting days, focus on consuming nutrient-dense, ketogenic-friendly meals.
Tips for Success:
- Plan and Prepare: Meal planning is essential for ensuring a well-balanced, ketogenic meal that meets your dietary requirements. Experiment with new recipes and explore plant-based alternatives to traditional high-carb ingredients.
- Monitor Nutrient Intake: Keep track of your macronutrient ratios, especially carbohydrates, proteins, and fats, to ensure you stay within the ketogenic range. Online food trackers or mobile apps can assist you in monitoring your nutrient intake.
- Stay Hydrated: Drink plenty of water throughout the day to stay hydrated and support overall well-being.
- Seek Professional Guidance: Consult with a registered dietitian or healthcare professional who specializes in plant-based nutrition and ketogenic diets. They can provide personalized guidance, address specific concerns, and help optimize your nutritional intake.
Conclusion: Following a vegan or vegetarian lifestyle doesn’t mean you have to forgo the benefits of a ketogenic diet with intermittent fasting. By carefully selecting plant-based fats, protein sources, and low-carbohydrate vegetables
and incorporating intermittent fasting, you can successfully adopt a ketogenic approach while aligning with your vegan or vegetarian values. Remember to consult with a healthcare professional or registered dietitian to ensure your dietary choices meet your nutritional needs and to discuss any specific concerns you may have.
By following these principles and incorporating a vegan or vegetarian ketogenic diet with intermittent fasting, you can achieve your weight loss goals, improve metabolic health, and potentially alleviate or reverse symptoms associated with chronic diseases. Embrace the power of plant-based nutrition and the ketogenic lifestyle to support your overall well-being and pave the way for a healthier future.
Author: Stephen Fitzmeyer, M.D.
Physician Informaticist
Founder of Patient Keto
Founder of Warp Core Health
Founder of Jax Code Academy, jaxcode.com
Connect with Dr. Stephen Fitzmeyer:
Twitter: @PatientKeto
LinkedIn: linkedin.com/in/sfitzmeyer/

Safeguarding Patient Privacy: The Crucial Intersection of Cybersecurity and HIPAA in Medicine and Health Informatics
Introduction
In the age of digital health, where electronic health records (EHRs) and telemedicine are becoming increasingly integral to the healthcare industry, the importance of safeguarding patient data is paramount. Cybersecurity and the Health Insurance Portability and Accountability Act (HIPAA) play pivotal roles in maintaining the privacy and security of healthcare information. In this article, we explore the crucial intersection of cybersecurity and HIPAA in medicine and health informatics.
Cybersecurity in Healthcare
Cybersecurity in healthcare is a complex and evolving field. It encompasses the measures and practices used to protect healthcare data from unauthorized access, breaches, and other malicious activities. With healthcare information becoming more digital, the stakes are higher than ever, as a breach can have severe consequences for both patients and providers. Here are some key aspects of cybersecurity in healthcare:
Data Encryption: Secure communication and data storage is vital. Encryption ensures that patient data remains confidential, even if intercepted.
Access Control: Restricting access to patient data is fundamental. Implementing role-based access controls ensures that only authorized personnel can access specific information.
Regular Audits and Monitoring: Continuous monitoring and regular audits help detect and address potential vulnerabilities in the healthcare system.
Incident Response: Being prepared for data breaches is critical. A robust incident response plan can minimize damage and protect patient data.
Employee Training: Human error is often the weakest link in cybersecurity. Training healthcare staff to recognize and prevent security threats is essential.
HIPAA and Its Role
HIPAA, enacted in 1996, is the cornerstone of patient data protection in the United States. It sets standards for the security and privacy of health information, regulates its transmission and storage, and imposes penalties for violations. HIPAA consists of two main rules:
Privacy Rule: This rule defines how patient information can be used and disclosed. It gives patients control over their health information and sets limits on its use by healthcare providers and others.
Security Rule: The Security Rule complements the Privacy Rule by establishing standards for the security of electronic health information. It outlines administrative, physical, and technical safeguards that covered entities must implement to protect health data.
The Intersection of Cybersecurity and HIPAA
Cybersecurity and HIPAA are intrinsically linked. HIPAA’s Security Rule compels healthcare organizations to implement specific cybersecurity measures to protect patient data. Compliance with the Security Rule is not optional; it is a legal obligation for any entity handling electronic protected health information (ePHI). Here’s how these two aspects intersect:
Security Safeguards: Healthcare providers must adopt cybersecurity practices that align with HIPAA’s technical safeguards, including access control, encryption, and audit controls.
Incident Response: HIPAA mandates that healthcare organizations have an incident response plan. Cybersecurity practices are essential in preparing for and mitigating breaches, which must be reported under HIPAA.
Penalties and Enforcement: HIPAA violations can result in significant fines. By following robust cybersecurity practices, healthcare organizations can reduce the risk of penalties and protect patient data.
Conclusion
In an era of technological innovation, the security and privacy of patient information in medicine and health informatics are non-negotiable. The intersection of cybersecurity and HIPAA serves as the linchpin for ensuring that healthcare organizations meet their ethical and legal obligations to protect patients’ most sensitive data. With the continued evolution of healthcare technology, it is imperative that healthcare providers remain vigilant in their commitment to cybersecurity and HIPAA compliance to maintain patient trust and data integrity in the digital age.

The First Step to Metabolic Health: Giving Up Seed Oils for Better Well-being
Introduction: In our pursuit of better health, we often focus on what we eat. We meticulously choose fresh produce, lean proteins, and whole grains. However, there’s one crucial ingredient hiding in many processed foods and restaurant meals that we need to pay attention to: seed oils. These commonly used cooking oils, such as soybean, canola, corn, and sunflower oils, have gained popularity but come at a cost to our metabolic health. Understanding their contribution to poor health and taking the first step of eliminating them from our diet can have significant benefits for our overall well-being.
The Problem with Seed Oils: Seed oils have become prevalent in the modern Western diet due to their affordability and high smoke point, making them ideal for cooking and food production. However, these oils are often highly processed and contain high levels of omega-6 fatty acids, which can disrupt the delicate balance of omega-6 to omega-3 ratio in our bodies. The overconsumption of omega-6 fatty acids, coupled with a deficiency in omega-3 fatty acids, has been linked to various health issues, including inflammation, obesity, insulin resistance, and cardiovascular diseases.
The Processing Method: To truly grasp the negative impact of seed oils on our health, it’s essential to understand the process by which they are manufactured. Most seed oils undergo a complex process involving extraction, refining, bleaching, and deodorizing. This process strips the oils of their natural antioxidants, vitamins, and minerals, leaving behind a product that is often rancid and devoid of any nutritional value. Additionally, the high heat and chemical solvents used during extraction can introduce harmful compounds, such as trans fats and free radicals, into the final product.
The First Step to Metabolic Health: Eliminating seed oils from our diet is a crucial first step towards achieving metabolic health. By replacing these unhealthy oils with healthier alternatives, such as extra virgin olive oil, coconut oil, avocado oil, or grass-fed butter, we can positively impact our well-being in several ways:
- Reduced Inflammation: Seed oils, with their imbalanced omega-6 to omega-3 ratio, promote inflammation in the body. By switching to healthier oils, we can restore the balance and alleviate chronic inflammation, which is a key driver of many chronic diseases.
- Improved Insulin Sensitivity: Seed oils have been associated with insulin resistance, a precursor to metabolic disorders like type 2 diabetes. Choosing healthier oils can help improve insulin sensitivity and support better blood sugar control.
- Enhanced Heart Health: Seed oils high in omega-6 fatty acids can negatively impact cardiovascular health by promoting inflammation, oxidative stress, and unhealthy cholesterol profiles. Opting for heart-healthy oils can lower the risk of heart disease and improve overall cardiovascular well-being.
- Nutrient-Rich Alternatives: Healthy oils like extra virgin olive oil and coconut oil offer a wealth of essential nutrients, antioxidants, and beneficial compounds that contribute to overall health. These oils can provide valuable health benefits and enhance the nutritional quality of our meals.
Conclusion: Taking the first step towards metabolic health involves eliminating seed oils from our diet. By understanding the detrimental effects of these oils on our well-being and opting for healthier alternatives, we can promote better metabolic function, reduce inflammation, and lower the risk of chronic diseases. Making this dietary change is a powerful choice that sets the stage for a healthier future. Remember to prioritize whole, unprocessed foods and consult with a healthcare professional or registered dietitian for personalized guidance on making healthier oil choices that align with your specific dietary needs and health goals.
Author: Stephen Fitzmeyer, M.D.
Physician Informaticist
Founder of Patient Keto
Founder of Warp Core Health
Founder of Jax Code Academy, jaxcode.com
Connect with Dr. Stephen Fitzmeyer:
Twitter: @PatientKeto
LinkedIn: linkedin.com/in/sfitzmeyer/

Unlocking the Potential: Exploring the Benefits of Taurine in Extending Life
In the pursuit of living longer, healthier lives, researchers and health enthusiasts alike are continuously exploring various strategies and supplements that may hold the key to longevity. One such compound that has captured the attention of scientists and health-conscious individuals is taurine. Widely recognized for its role in energy metabolism and overall health, taurine is an amino acid that offers a range of potential benefits, including its ability to extend life. In this article, we delve into the fascinating world of taurine and its potential as a longevity-enhancing compound.
Taurine, often referred to as a “wonder molecule,” is naturally produced in the body and is found abundantly in various tissues, including the heart, brain, and muscles. It plays a crucial role in numerous physiological processes, such as regulating cell membrane stability, supporting antioxidant activity, modulating neurotransmission, and aiding in the proper functioning of vital organs. These multifaceted functions contribute to its potential in promoting longevity.
One of the key mechanisms through which taurine may extend life is its ability to combat oxidative stress and inflammation. As we age, our bodies accumulate damage from free radicals and experience increased inflammation, which contribute to the aging process and the development of age-related diseases. Taurine acts as a potent antioxidant, neutralizing free radicals and reducing oxidative stress. Additionally, it exerts anti-inflammatory effects, helping to mitigate chronic inflammation that can accelerate aging and increase the risk of age-related conditions.
Furthermore, taurine has been shown to support cardiovascular health, which is closely linked to longevity. It helps maintain healthy blood pressure levels, improves lipid profiles by lowering cholesterol and triglyceride levels, and enhances the function of blood vessels. By promoting cardiovascular wellness, taurine may reduce the risk of heart disease and other cardiovascular complications, ultimately contributing to a longer and healthier life.
The benefits of taurine extend beyond cardiovascular health. Research suggests that it may also support brain function and mental well-being, another crucial aspect of healthy aging. Taurine has been shown to enhance cognitive performance, protect against neurodegenerative diseases, and improve mood and sleep quality. By supporting optimal brain health, taurine may help maintain cognitive function and overall mental vitality as we age.
Additionally, taurine’s role in energy metabolism and exercise performance is worth noting. It aids in the production of cellular energy by supporting the function of mitochondria, the powerhouse of our cells. This energy-boosting effect may contribute to maintaining an active lifestyle and promoting physical fitness, both of which are linked to longevity and overall well-being.
While taurine is naturally present in certain foods, such as meat, seafood, and dairy products, some individuals may benefit from taurine supplementation to ensure optimal levels. As with any supplement, it is important to consult with a healthcare professional before starting taurine supplementation, especially if you have any underlying health conditions or are taking medications.
In conclusion, taurine holds immense promise as a compound that may contribute to extending life and promoting healthy aging. Its antioxidant, anti-inflammatory, cardiovascular, cognitive, and energy-enhancing properties position it as a potential longevity-enhancing supplement. However, further research is needed to fully understand its mechanisms and establish optimal dosage recommendations.
As the quest for longevity continues, taurine presents itself as a compelling area of exploration and potential intervention. Embracing a holistic approach to health, including a balanced diet, regular exercise, and informed supplementation, may help unlock the remarkable benefits of taurine and pave the way for a longer, healthier, and more vibrant life.
Disclaimer: The information in this article is intended for informational purposes only and should not be interpreted as medical advice. It is always recommended to consult
with a healthcare professional before making any changes to your diet, lifestyle, or supplementation routine. They can provide personalized guidance based on your specific health needs and considerations.
Remember, while taurine shows promise in extending life and promoting health, it is just one piece of the puzzle in the complex journey of aging gracefully. Adopting a comprehensive approach to overall wellness, including maintaining a nutritious diet, engaging in regular physical activity, managing stress levels, getting adequate sleep, and staying socially connected, is essential for optimal health and longevity.
As the scientific community continues to delve deeper into the potential benefits of taurine and other compounds, it is an exciting time to explore the possibilities of enhancing our well-being and extending our lifespan. By staying informed, making informed choices, and working closely with healthcare professionals, we can strive to lead longer, healthier, and more fulfilling lives.
Please note that individual responses to taurine may vary, and it is important to consider your specific health status and any existing medical conditions before incorporating taurine or any other supplement into your routine.
Author: Stephen Fitzmeyer, M.D.
Physician Informaticist
Founder of Patient Keto
Founder of Warp Core Health
Founder of Jax Code Academy, jaxcode.com
Connect with Dr. Stephen Fitzmeyer:
Twitter: @PatientKeto
LinkedIn: linkedin.com/in/sfitzmeyer/
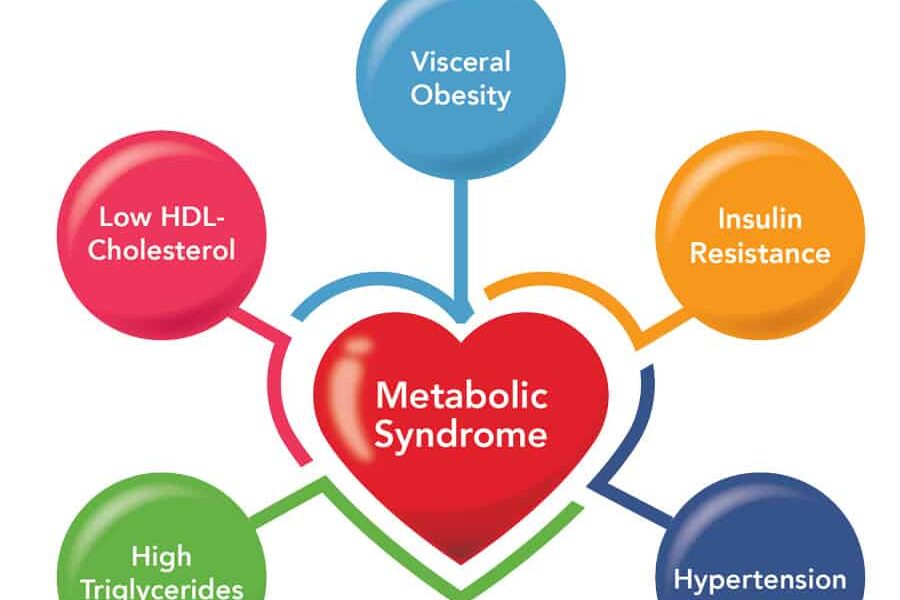
Taking Control of Your Health: Combating Metabolic Syndrome with Keto and Intermittent Fasting
Introduction: Metabolic syndrome has reached alarming levels in the United States, with a staggering 88% of the adult population affected. This condition not only poses immediate health risks but also increases the likelihood of developing chronic diseases in the future. However, by adopting a combination of the ketogenic diet (keto) and intermittent fasting (IF), you can take proactive steps to regain control of your health and prevent the onset of chronic diseases that have plagued previous generations.
The Metabolic Syndrome Epidemic: Metabolic syndrome is a cluster of interconnected metabolic abnormalities that include abdominal obesity, high blood pressure, elevated blood sugar levels, and abnormal lipid profiles. This dangerous combination significantly increases the risk of heart disease, type 2 diabetes, stroke, and other chronic conditions. The prevalence of metabolic syndrome in the U.S. highlights the urgent need for effective strategies to address this health crisis.
The Power of the Ketogenic Diet (Keto): The ketogenic diet is a low-carbohydrate, high-fat eating plan that promotes ketosis, a metabolic state in which the body primarily burns fat for fuel. By drastically reducing carbohydrate intake and increasing healthy fats, the keto diet helps regulate blood sugar levels, promote weight loss, and improve insulin sensitivity, all of which are crucial in combating metabolic syndrome. Keto can also lead to a shift in the body’s fuel source, reducing reliance on carbohydrates and promoting fat burning, which can aid in weight management and reducing abdominal obesity.
Intermittent Fasting (IF) for Metabolic Health: Intermittent fasting involves cycling between periods of eating and fasting. This approach not only helps control calorie intake but also promotes metabolic flexibility and enhances various health benefits. IF can improve insulin sensitivity, reduce inflammation, and promote weight loss. It also stimulates autophagy, a natural cellular cleansing process that helps remove damaged cells and supports overall cellular health. By incorporating IF alongside the ketogenic diet, you can further enhance the positive impact on metabolic syndrome and long-term health.
Breaking the Cycle: One of the most significant advantages of adopting a proactive approach to your health through keto and IF is the ability to break the cycle of chronic diseases that have affected previous generations. By making lifestyle changes now, you can prevent the onset of conditions like type 2 diabetes, heart disease, and obesity, which have plagued your parents or family members. Taking control of your health empowers you to pave a different path and avoid the struggles and limitations associated with chronic diseases.
Embracing a Healthier Future: Combating metabolic syndrome with keto and IF requires commitment and dedication, but the rewards are well worth the effort. Alongside the metabolic benefits, you may experience weight loss, increased energy levels, improved mental clarity, and a reduced risk of chronic diseases. It’s important to consult with healthcare professionals or registered dietitians to ensure your keto and IF practices are suitable for your individual health needs.
By taking control of your health now, you have the opportunity to rewrite your future. Don’t let metabolic syndrome and chronic diseases define your life. Embrace the power of keto and IF as tools to optimize your metabolic health, reclaim your vitality, and build a foundation for long-term well-being. Make a conscious choice today to break free from the statistics and create a healthier future for yourself and generations to come.
Author: Stephen Fitzmeyer, M.D.
Physician Informaticist
Founder of Patient Keto
Founder of Warp Core Health
Founder of Jax Code Academy, jaxcode.com
Connect with Dr. Stephen Fitzmeyer:
Twitter: @PatientKeto
LinkedIn: linkedin.com/in/sfitzmeyer/